
Signs of dehydration in school-age children are easy to miss. Kids between 4 and 10 are active, playful, and rarely stop to drink water. Their bodies lose fluids faster than adults, and thirst often appears late. Whether from illness or hours in the sun, dehydration can develop quickly.
Warning signs include dark urine, dry lips, tiredness, irritability, headache, dizziness, reduced urination, and no tears when crying. Because thirst is a late signal, a child may already be 2–3% dehydrated before they mention feeling thirsty.
By then, subtle changes like fatigue or mood shifts are often noticeable. Recognizing these clues early helps parents keep children healthy, energetic, and safe at school, on the playground, or while recovering from illness. In this guide, you’ll learn how to spot dehydration early and respond quickly to keep your child safe.
Why Signs of Dehydration in School-Age Children Appear Faster Than in Adults
To recognize the signs of dehydration in school-age children, we first have to understand how their bodies process water differently from ours. Because their physiology is still developing, fluid loss can happen faster than many parents realize. Here’s why:
- Higher Surface-Area-to-Mass Ratio: Children have more skin surface area compared to their body weight than adults. This means they absorb heat faster and lose fluids more quickly through breathing and evaporation—even without heavy sweating.
- Inefficient Sweating Mechanisms: In children aged 4–10, sweat glands are still maturing. They do not start sweating as early as adults, which causes their core temperature to rise faster, increasing the risk of heat exhaustion and fluid loss.
- Higher Metabolic Rate: Growth and high energy levels mean a child’s metabolic rate is significantly higher than an adult’s. Every activity increases fluid demand, which can gradually deplete reserves over a busy school day.
- The “Thirst Lag” Phenomenon: Research shows children often don’t feel thirsty until they are already 2–3% dehydrated. By the time they ask for water, fatigue, irritability, or headaches may already be present.
- Increased Risk During Illness: Because their fluid reserves are smaller, even short episodes of sweating, vomiting, diarrhea, or fever can drain water quickly—sometimes within hours.
- Environmental & Behavioral Factors: Hot classrooms, outdoor activities, or long stretches without breaks can quickly drain their fluid reserves. Unlike adults, kids rarely recognize early signs of dehydration, which makes proactive hydration important.
Signs of Dehydration in School-Age Children: 10 Critical Symptoms (Ages 4–10)
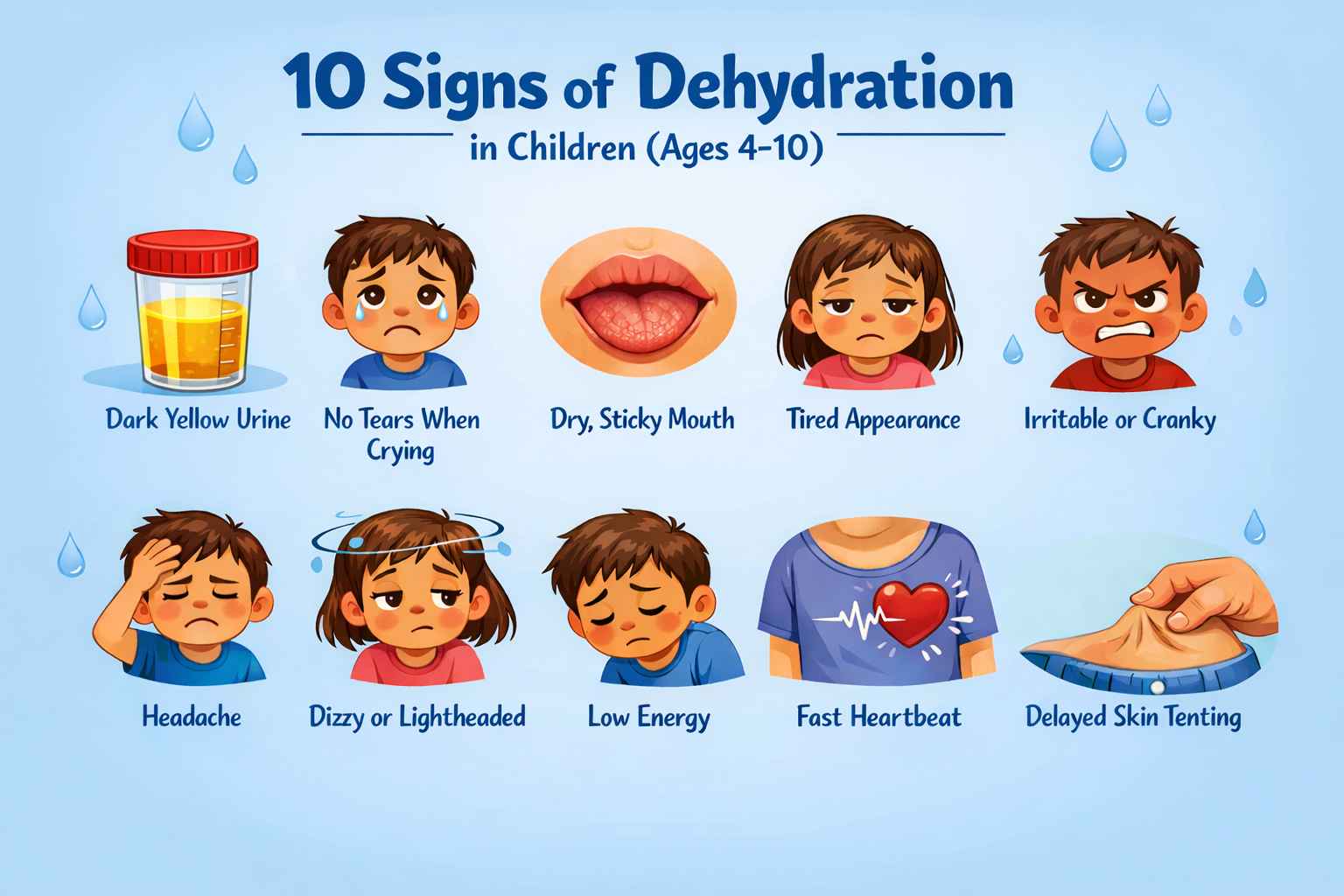
Here are the 10 most important signs of dehydration in children ages 4–10. These common symptoms of dehydration in children often appear before a child says they are thirsty.
1. Dark Yellow Urine (The “Apple Juice” Sign)
In a well-hydrated child, urine should be pale yellow, similar to diluted lemonade.
- Red flag: If it looks dark yellow, amber, or tea-colored, the kidneys are concentrating urine to conserve water. This is often the earliest and most reliable sign of mild dehydration in children.
- Frequency check: A school-age child should urinate at least 4 to 5 times per day. If they have not gone for 6 to 8 hours, especially during illness, dehydration should be considered.
2. No Tears When Crying
This is one of the most important signs for parents to see. When fluid levels drop, the body prioritizes circulation to vital organs over tear production.
- What to notice: If your child is crying but producing very few or no tears, it may be a sign of moderate dehydration.
- Clues: This sign is especially concerning if paired with dry lips and reduced urination.
3. Dry, Sticky Mouth
A quick look inside your child’s mouth can reveal a lot.
- Healthy mouth: Moist, shiny tongue and cheeks.
- Dehydrated mouth: Saliva becomes thick, sticky, or “ropey.” The tongue may look dry, and lips may crack.
- Why it matters: This is often an early physical sign that appears before more serious symptoms develop.
4. Tired Appearance
Dehydration often shows up in a child’s face before anywhere else.
- What to notice: Hollow cheeks, droopy eyelids, or a pale, “washed-out” look can make a child seem more tired than usual.
- Why it matters: Parents often mistake this for simple fatigue, but it’s actually the body signaling low fluid levels and reduced energy reserves.
5. Irritability or Sudden Mood Changes
Even mild dehydration can affect a child’s attention, mood, and behavior.
- Early signs: A child may become unusually cranky, struggle to concentrate, or lose patience with simple tasks.
- What to watch for: Sudden emotional meltdowns or unexpected irritability often appear before a child even feels thirsty.
6. Headache After School or Sports
Headaches are one of the most common—and often overlooked—signs of dehydration in school-age children.
- When it shows up: Many kids complain of headaches after a long school day, outdoor play, or sports practice.
- Why it happens: Reduced fluid levels make the blood thicker, forcing the heart to work harder. This strain can trigger painful changes in blood vessels, leading to headache discomfort.
7. Dizziness or Lightheadedness
If your child says the room feels like it’s spinning or they look unsteady when standing up, dehydration may be interfering with blood pressure regulation.
- Why it happens: Fluid loss reduces the amount of circulating blood volume. When a child changes position—like standing up quickly—less blood reaches the brain for a moment, causing dizziness or wobbly legs.
- What it means: This is more than just “getting up too fast.” It’s a warning sign that hydration needs attention.
⚠️ Important Note: If dizziness is persistent or paired with other signs like rapid heartbeat or extreme fatigue, fluids should be offered immediately and medical evaluation may be necessary.
8. Unusual Fatigue or Low Energy
There is a noticeable difference between normal tiredness and dehydration-related fatigue.
- Early signs: A mildly dehydrated child may seem sluggish, quieter than usual, or less interested in play and routine activities.
- More concerning: Extreme lethargy, where the child appears floppy, unusually drowsy, or difficult to engage, signals that the body is slowing down to protect vital organs. This level of fatigue is a hallmark of severe dehydration in children.
⚠️ Important Note: While mild fatigue can often be corrected with fluids, severe lethargy should be taken seriously and assessed promptly by a healthcare professional.
9. Rapid Heartbeat at Rest
When fluid volume drops, the heart works harder to maintain circulation.
- What to notice: If your child is sitting quietly but their heartbeat feels unusually fast—almost like they’ve just finished running—it may be linked to dehydration.
- Clues to watch for: A racing pulse alongside other signs such as dry mouth or reduced urination strengthens the concern.
- When to act: Persistent rapid heart rate should always be checked by a healthcare professional, as it can signal more serious fluid loss or another underlying issue.
10. Delayed Skin Tenting
This is a simple clinical check you can do at home. Gently pinch a small fold of skin on your child’s abdomen, hold it for one to two seconds, then release.
- Normal result: Hydrated skin snaps back instantly, like a rubber band.
- Dehydrated result: The skin stays “tented” or moves back slowly, showing a loss of elasticity from fluid depletion.
⚠️ Important Note: This test should never be used in isolation. Always interpret it alongside other signs—such as urine color, energy levels, and tear production—for a complete picture of your child’s hydration status.
How Much Water Do Kids Actually Need? (Ages 4–10)
Fluid needs increase with age, activity level, and body weight within the 4–10 range. There isn’t a strict one-size-fits-all number. Requirements vary based on size, physical activity, weather, and overall health. However, pediatric guidelines provide parents with a reliable daily baseline.
The Daily Hydration Baseline
A child’s total fluid intake should be about 40–50 milliliters per kilogram of body weight per day.
Weight Examples:
- A 20 kg child → 800–1,000 mL (0.8–1 liter) per day
- A 30 kg child → 1.2–1.5 liters per day
Age Examples:
- Ages 4–8 → About 5 glasses (~1.2 L) per day
- Ages 9–10 → About 6–7 glasses (~1.4–1.6 L) per day
When More Fluids Are Needed
The baseline applies to normal weather and regular activity. Children need additional fluids in situations such as:
- Fever
- Vomiting or diarrhea
- Hot weather
- Sports or heavy physical activity
In those situations, additional fluids are required beyond the baseline calculation.
What are the Best Fluids for Dehydrated Children?
When treating dehydration in school-age children, your goal is to restore both water and essential electrolytes, specifically sodium and potassium.
Using only plain water during an illness can sometimes dilute the body’s remaining minerals, making an imbalance worse. Here are the best options:
1. Plain Water (For Everyday Hydration)
Water is the simplest way to maintain daily hydration. It is the gold standard for children who are active but otherwise healthy.
- How it Works: Restores fluid volume in the blood but does not replace salts lost during sweating, vomiting, or fever.1
- How to Use: Offer small, frequent sips throughout the day. Encourage drinking before, during, and after activity—even if the child does not feel thirsty.
Note: Water alone is often insufficient for illness-related dehydration. If a child is losing fluids via illness, they need an electrolyte boost to stay safe.
2. The Gold Standard: Oral Rehydration Solutions (ORS)
The World Health Organization recommends ORS (such as Pedialyte) as the first-line treatment for dehydration caused by illness (vomiting or diarrhea or fever).
- How it Works: It uses a precise ratio of glucose and sodium to trigger a “co-transport” mechanism. This essentially “fast-tracks” water into the bloodstream much faster than water alone.
- How to Use: Aim for 50–100 mL per kilogram of body weight over 4 hours, given in small, frequent sips.
Note: ORS is the safest choice for moderate dehydration due to diarrhea, vomiting, or fever.
3. Diluted Apple Juice
For children over 24 months with mild dehydration symptoms, diluted apple juice is a scientifically backed alternative.
A study published in NCBI found that for children with mild gastroenteritis and mild dehydration, giving diluted apple juice first, followed by their favorite fluids, helped reduce the need for IV fluids compared to using only ORS.2
- How it Works: The sugar provides quick energy, and the familiar taste helps children drink more. Diluting it is critical, as full-strength juice has too much sugar, which can actually pull water into the gut and worsen diarrhea.
- How to Use: Mix 50% apple juice with 50% water. Offer small, frequent sips.
Note: Diluted apple juice is appropriate only for mild dehydration. For moderate dehydration or ongoing vomiting, ORS remains the safer and preferred option.
4. Coconut Water
Coconut water helps replenish fluids lost during exercise, outdoor heat exposure, or mild fluid loss.
- How it Works: Studies found that coconut contains potassium, magnesium, calcium and some carbohydrates. These nutrients help replace certain electrolytes lost through sweat. However, its sodium content is relatively low.3,4
- How to Use: Serve chilled for better palatability. It can be mixed with a pinch of sea salt to boost its sodium content if the child has been sweating heavily.
Note: Due to its low sodium content, coconut water is only best for mild fluid loss from sweat, not for medical dehydration from stomach infections such as diarrhea and vomiting.
Fluids to Avoid During Dehydration
Not all drinks help when a child is dehydrated. In fact, some can make fluid loss worse by increasing sugar load or acting as diuretics.
- Energy drinks
- Highly caffeinated beverages
- Undiluted fruit juices
- Soda
- Very sugary sports drinks
Note: These drinks are high in sugar or caffeine. As a result, they can pull water into the intestine, worsen diarrhea, and increase fluid loss instead of fixing it.
When to See a Doctor: Mild vs Moderate vs Severe
| Level of Dehydration | Approx. Fluid Loss | Key Signs | Parent Action |
|---|---|---|---|
| Mild | ~3–5% body weight | • Dark yellow urine • Urinating slightly less than usual • Dry lips or mildly dry mouth • Mild headache • Slight irritability or tired look | Offer fluids (water, diluted juice, or ORS). Monitor closely. |
| Moderate | ~6–9% body weight | • No tears when crying • Very dry mouth or sticky saliva • Urinating fewer than 3–4 times/day • Dizziness when standing • Rapid heartbeat at rest • Noticeable fatigue or low energy | Give Oral Rehydration Solution (ORS). Seek medical advice if symptoms persist or worsen. |
| Severe | ≥10% body weight (Medical Emergency) | • Extreme drowsiness or floppy appearance • Very little or no urine for 8 hours • Sunken eyes or hollow cheeks • Skin pinch test stays tented • Rapid pulse, confusion, fainting | Seek immediate medical care. Severe dehydration requires urgent treatment, often IV fluids. |
How to Prevent Dehydration
Prevention is about creating a “hydration-friendly” environment so children don’t have to rely on their underdeveloped thirst cues.
- The “Lemonade” Rule: Teach your child to check their urine. If it looks like dark apple juice, they need to drink a full glass of water immediately. If it looks like pale lemonade, they are doing great.
- Scheduled Water Breaks: During sports or outdoor play, don’t wait for them to ask. Mandate a “water reset” every 20 minutes. A school-age child should aim for 3–5 ounces of fluid during these breaks.
- Hydrate Through Food: Supplement water intake with high-moisture snacks. Watermelon, cucumbers, strawberries, and oranges are roughly 90% water and provide a refreshing way to stay hydrated.
- Accessible Gear: Ensure your child has a reusable water bottle they can open easily. Kids are more likely to drink when the water stays cold and the bottle is “cool” to carry.
- Pre-Hydrate Before Activity: If you know your child has a soccer game or a day at the park, encourage them to drink a glass of water before leaving the house.
Key Takeaway
Recognizing the signs of dehydration in school-age children is one of the most important steps parents can take to protect their child’s health.
Kids aged 4–10 often miss early thirst cues, and by the time they ask for water, they may already be dehydrated. Simple checks like urine color, energy levels, and the skin pinch test can help parents act quickly.
With scheduled water breaks, hydration-friendly snacks, and the right fluids such as ORS, children can stay healthy, active, and safe every day.
The Big Three for Parents:
- Look for subtle shifts: irritability, headaches, unusual tiredness.
- Use gold standard checks: urine color and skin pinch test.
- Act fast: Everyday hydration can be managed with water, but when illness strikes (fever, vomiting, or diarrhea), ORS is the gold standard. Apple juice and coconut water may help in mild cases or heat related dehydration only.
Frequently Asked Questions About Dehydration in School-Age Children
Q1. What are the first signs of dehydration in children?
Early signs include dark yellow urine, a dry mouth, irritability, headaches, and unusual tiredness. However, children often do not feel thirsty until they are already mildly dehydrated. Therefore, waiting for thirst is not always reliable.
Q2. How can parents check for dehydration at home?
A simple way to check at home is the skin pinch test. Gently pinch the skin on the abdomen, then release it.
If the skin does not return to normal quickly, dehydration may be present. In addition, check urine color and frequency, along with your child’s energy level. Looking at all signs together gives a clearer picture.
Q3. What is the best fluid for dehydration in children?
The gold standard is Oral Rehydration Solution (ORS). It contains the right balance of sugar and salt to help the body absorb fluids quickly and safely.
For very mild dehydration caused by heat or activity, diluted apple juice or coconut water may help. However, during illness such as vomiting or diarrhea, ORS is the safest and most effective option.
Q4. When should I call a doctor for dehydration?
Contact your doctor if you notice moderate signs such as no tears when crying, persistent dizziness, or very low urine output.
Seek emergency care immediately if your child shows severe symptoms, including extreme drowsiness, a floppy appearance, a rapid resting heartbeat, confusion, or no urination for more than 8 hours.
Q5. Can plain water alone treat dehydration?
Plain water is excellent for everyday hydration. However, during illness, children lose both fluids and electrolytes such as sodium and potassium.
Drinking only water can dilute these remaining electrolytes further. As a result, recovery may be slower. In these situations, ORS is necessary to restore proper balance.
Q6. What fluids should be avoided?
Avoid energy drinks, soda, undiluted fruit juices, and caffeinated beverages. These are often too high in sugar, which can pull more water into the gut and worsen diarrhea, or contain caffeine, which may increase fluid loss through urination.
References
📚 Click to view references
- Faizan U, Rouster AS. Nutrition and Hydration Requirements In Children and Adults.
StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK562207/
- World Health Organization. Diarrhoeal disease. 2023.
Available from: https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease
- Freedman SB, et al. Effect of Dilute Apple Juice and Preferred Fluids vs Electrolyte Maintenance Solution on Treatment Failure Among Children With Mild Gastroenteritis.
JAMA. 2016;315(18):1966-74. Available from: https://pubmed.ncbi.nlm.nih.gov/27131100/
- Kalman DS, et al. Comparison of coconut water and a carbohydrate-electrolyte sport drink on measures of hydration. J Int Soc Sports Nutr. 2012;9:1. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3293068/
- O’Brien BJ, et al. Coconut Water: A Sports Drink Alternative? Sports (Basel). 2023;11(9):183.
Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10534364/